

BMJ|NHS hospital capacity during covid-19
BMJ|NHS hospital capacity during covid-19
Some shocking data demonstrating low ICU attendance in 2020 with the abandonment of healthcare for millions during lockdown.

ICU
English ICU occupancy before the pandemic was 75-88% despite bed numbers increasing. On 30 January 2020, the day the World Health Organization declared covid-19 to be a public health emergency of international concern, there were 3,654 adult critical care beds in acute hospitals in England, of which 3044 (83%) were occupied.
Ventilators
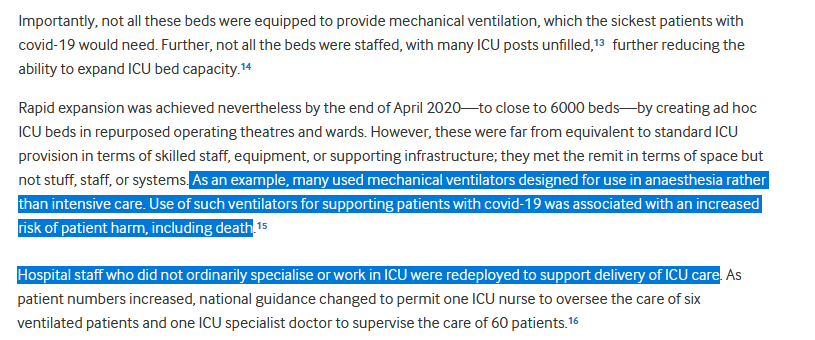
The expansion of ICU beds during April 2020 to create 6,000 beds placed patients at increased risk of death due to inadequate equipment being used with untrained staff deployed to look after the sickest patients.
‘‘Many used mechanical ventilators designed for use in anaesthesia rather than intensive care….
‘‘Use of such ventilators for supporting patients with covid-19 was associated with an increased risk of patient harm, including death.’’
ICU Capacity
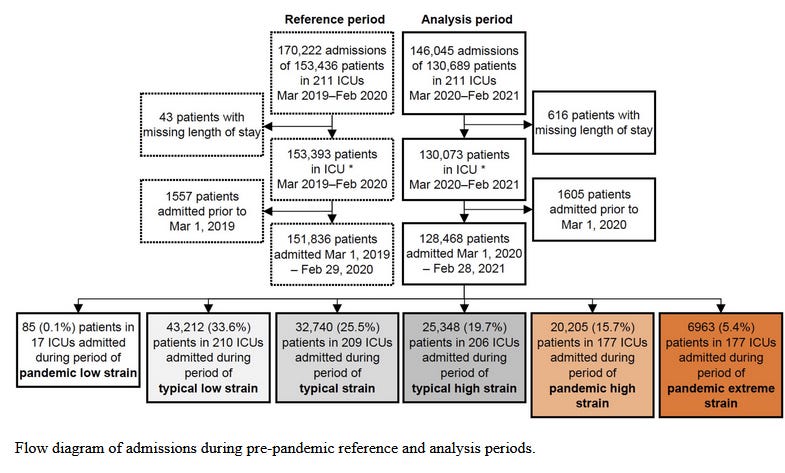
As can be seen pre ‘pandemic’ …ICU’s in England experienced 170,222 admissions with 153,436 patients in ICUs. Period Mar 2019-Feb 2020.
During the peak of the ‘pandemic’ 146,045 with 130,689 in ICUs. Period Mar 2020-Feb 2021.
To increase the death rate?
Many hospitals experienced shortages of staff, medicines, equipment, and other essential supplies, including oxygen. In one hospital, oxygen supply problems were so severe that it was forced to declare a major incident and transfer patients to neighbouring hospitals.
Advanced respiratory therapies such as continuous positive pressure ventilation are—for patient safety—normally delivered in an ICU or other specialised setting. During the pandemic, many thousands of patients received such treatments outside ICU, cared for by medical teams with even more sparse staffing.
Transferring critically ill patients between units to ease capacity pressures (capacity transfers) is a substantial logistic challenge, requiring specialist staff and equipment. A multicentre review found that serious adverse events occur in up to 8.9% of critical care transfers.
Post ‘vaccination’
‘‘In the winter before the pandemic, from December 2019 to February 2020, only 68 capacity transfers took place, but between December 2020 and February 2021, this increased 30-fold to 2,152.’’
Although much discussion focuses on spring 2020, the wave experienced from December 2020 to February 2021 brought an even larger surge. Official data show an astonishing peak occupancy of 5,702 ICU beds in England during this period. It was not until 6 March 2021 that ICU occupancy consistently fell below 4,000 in England: still higher than total ICU capacity in early 2020.
Surgical backlogs
A a reduction in non-urgent NHS care was an inevitable consequence of ‘‘covid-19-’’related pressure. Elective operations were suspended.
The effect of ‘‘covid-19’’ surges on anaesthetic and surgical procedures was best illustrated by a survey of UK hospitals in January 2021 by the Royal College of Anaesthetists:
53% reported that covid-19 pressures substantially prevented them from providing anaesthetic services
38% described anaesthetic care as hampered, and…
‘‘only 9% were able to provide close to normal services.’’
More than 2000 anaesthetists were unavailable for theatre work.
75% were redeployed to ICU.
42% of UK NHS operating theatres were closed, with throughput almost halved in those remaining open.
Routine adult non-cancer surgery ran at 33% of pre-pandemic levels.
Cancer surgery at 61%, and paediatric surgery at 32%….
‘‘Overall, more than half of surgical activity was lost—close to 10,000 operations every day.’’
Learning from the crisis
The study ends with an interesting bit of crystal ball gazing.
‘‘The threat from covid-19 for NHS hospitals has receded but not entirely disappeared. Pandemics will inevitably be more frequent in the future.’’
‘‘Inevitably’’???
End
Links:
https://www.bmj.com/content/385/bmj-2023-075613
https://journals.lww.com/ccmjournal/pages/imagegallery.aspx?year=2022&issue=06000&article=00024